PA consults Facebook for help treating her patient's pulmonary embolism
💬 comments
We're going to need a thrombectomy after reading this post.

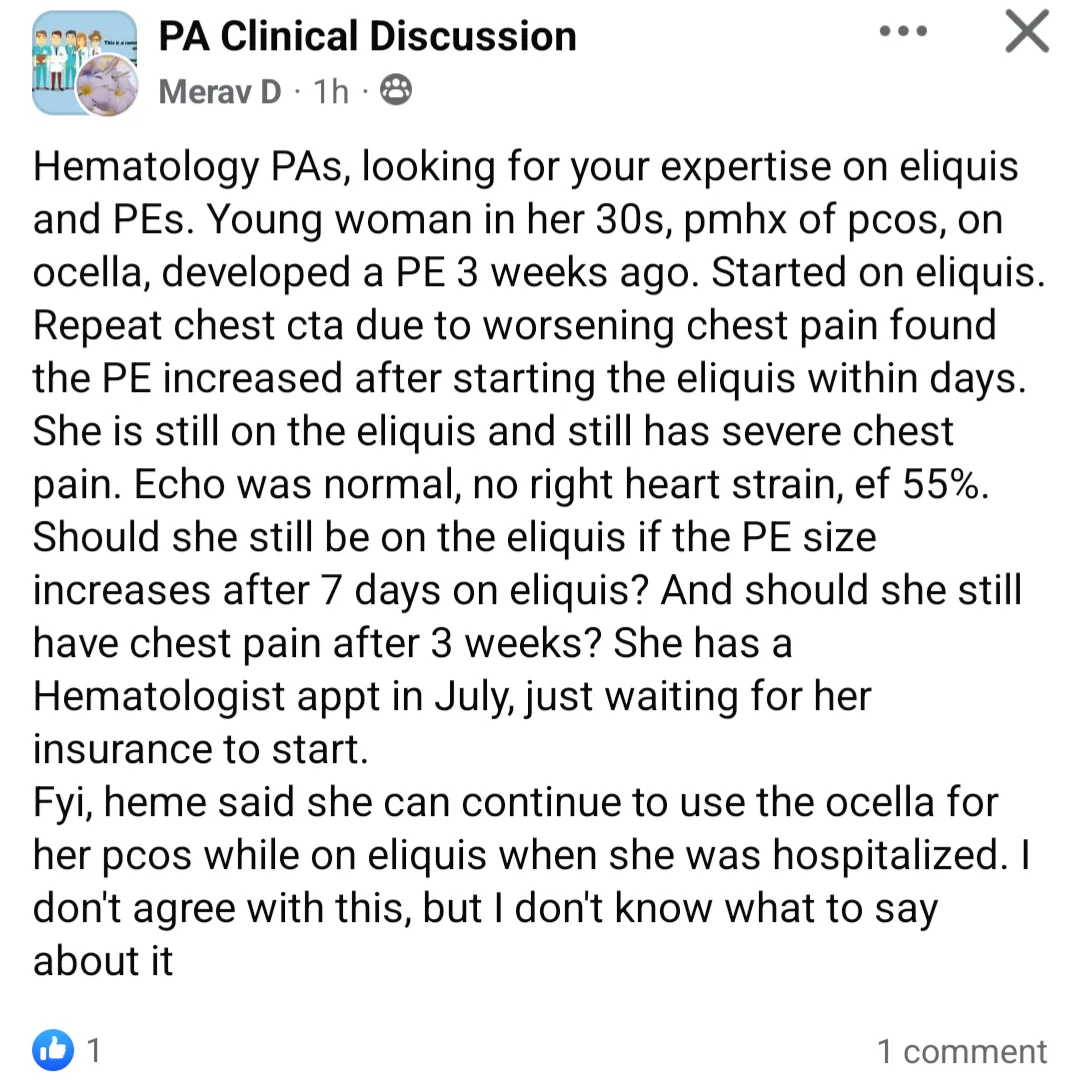
Quality over quantity is the name of the game here at MidlevelWTF. But because we currently have a backlog of content so long and girthy that it would put the world's biggest piece of human shit to shame, we endeavor to push out only the best pieces of crap we can find. Today's steaming turd of a post comes from New York City-based physician assistant "Merav D" (Merav Darzi, New York PA license #020365) in the "PA Clinical Discussion" Facebook group. Ms. Darzi comes across as a bit flustered as she describes her patient - a young woman in her 30s who developed a pulmonary embolism (PE) 3 weeks ago, (still) on an oral estradiol-based contraceptive (Ocella) that is generally contraindicated in patients with a pulmonary embolism, and is now having worsening chest pain with repeat CT angiography (CTA) showing an increase in size of said pulmonary embolism despite treatment with oral anticoagulation (Eliquis).

Ms. Darzi would like to know, "Should she still be on the eliquis if the PE size increases after 7 days on eliquis?" "And should she still have chest pain after 3 weeks?" Well, we're no fucking geniuses here, let alone hematologists, but you don't need to be a fucking physician to appreciate the fact that if your patient's symptoms are getting worse despite your treatment, then maybe your "treatment" isn't fucking working. Who in the world would have guessed that treatment failure with direct oral anticoagulants (DOACs) like Eliquis and Xarelto is actually a known clinical phenomenon?
 Graham McIlroy
Graham McIlroy James Rankin
James RankinWe're not sure why "heme said she can continue to use the ocella for her pcos while on eliquis when she was hospitalized". Maybe the "heme" she talked to was really a midlevel nurse practitioner cosplaying as a board-eligible/board-certified physician? Was OB/GYN ever consulted for alternative contraceptive options? An actual hematologist who previewed this post before publication wisely suggested "don’t fuck around with PEs" and admitting the patient for a heparin drip and switching to Coumadin, an opinion also supported by a critical care physician. At least Ms. Darzi doesn't seem to agree with the idea of continuing Ocella, although she doesn't know "what to say about it". Well, in any case, here's what we have to fucking say about it: it's not like having a huge honking blood clot in your lungs with "worsening chest pain" while continuing to take an estradiol-containing oral contraceptive is potentially lethal or anything. Yeah, let's just consult some random fucking "hematology PAs" on Facebook and wait for the equally clueless peanut gallery to chime in. What's Ms. Darzi's apparent plan for the patient in the meantime? "She has a hematologist appt in July, just waiting for her insurance to start." Well, don't mind us, we'll be over here twiddling our thumbs until this poor patient dies from cardiopulmonary arrest.