A rare case of "Perry orbital cellulitis"
💬 comments
No worries, we can just refer the patient to a "red eye" optometrist with whom we have an "informal arrangement"!
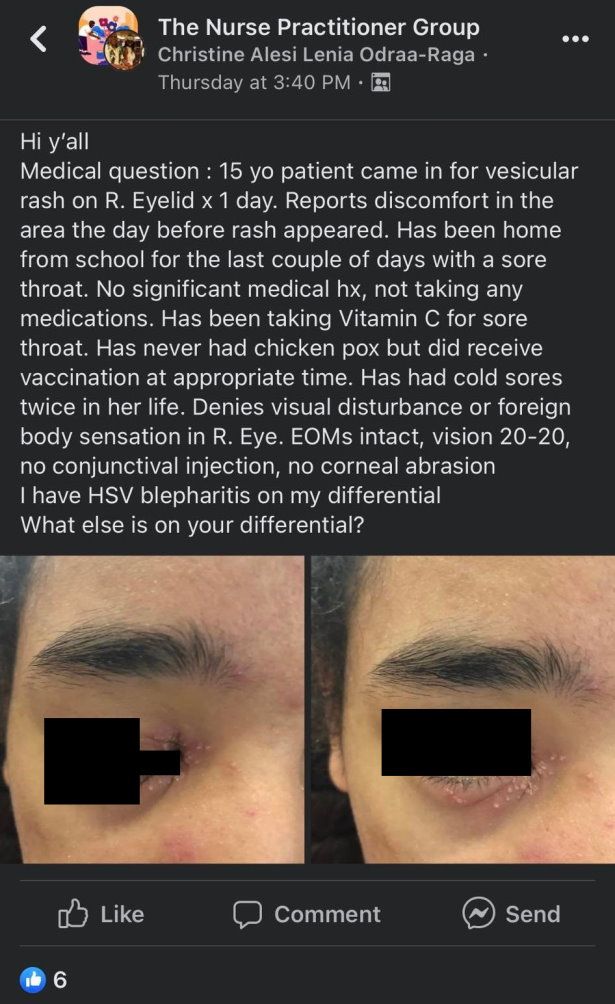
As the old saying goes, hindsight is 20/20, but when a midlevel nurse practitioner not only posts an ophthalmological complaint on Facebook but explicitly asks the peanut gallery for a crowdsourced differential diagnosis, it might as well be legally blind. Case in point: this eye-opening post by "Christine Alesi Lenia Odraa-Raga" (who actually appears to be a physician assistant, not a nurse practitioner), and the resulting trainwreck of a comment section it spawned. As Christine didn't have the common courtesy to avoid a potential HIPAA violation and posted full shots of the patient's eyes, we have censored them here to preserve the poor patient's privacy.
Notwithstanding the fact that Christine's differential diagnosis apparently consists of only one thing, the idea that this could be HSV blepharitis is questionable at best. Given the lack of associated ocular symptoms, absence of periocular edema, and presence of the "rash" on the midface, and sudden onset, the likelihood that this is a true blepharitis is low, let alone blepharitis due to HSV. But, as we shall see, the real geniuses can be found in the comment section.
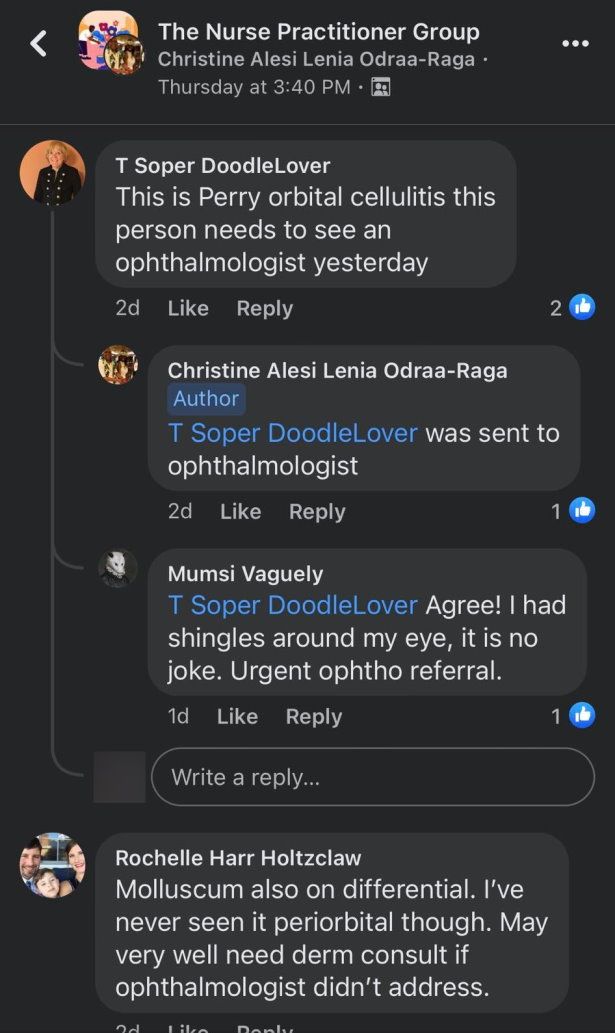
Coming in hot is "T Soper Doodlelover", or DNP Tracey Soper, with the slam-dunk diagnosis of "Perry orbital cellulitis". First of all, who the fuck is Perry and why does he have cellulitis? Joking aside, we'll give Ms. Soper, who teaches at the highly reputable diploma mill institution known as Walden University, the benefit of the doubt and assume that she's referring to periorbital (preseptal) cellulitis. This also happens to be a questionable diagnosis given the absence of eyelid swelling and atypical appearance of the pictured lesion. While the suggestion to refer to an ophthalmologist is not entirely unreasonable (better safe than sorry when you're dealing with a clueless midlevel and an eye complaint, right?), treatment for a run-of-the-mill case of true periorbital cellulitis (i.e. no orbital involvement) could be reasonably initiated on an outpatient basis by a primary care physician or emergency physician.
Oh, what perfect timing! Time to give a shout-out to one of our favorite papers showing that midlevels order shittier, lower-quality referrals compared to physicians.

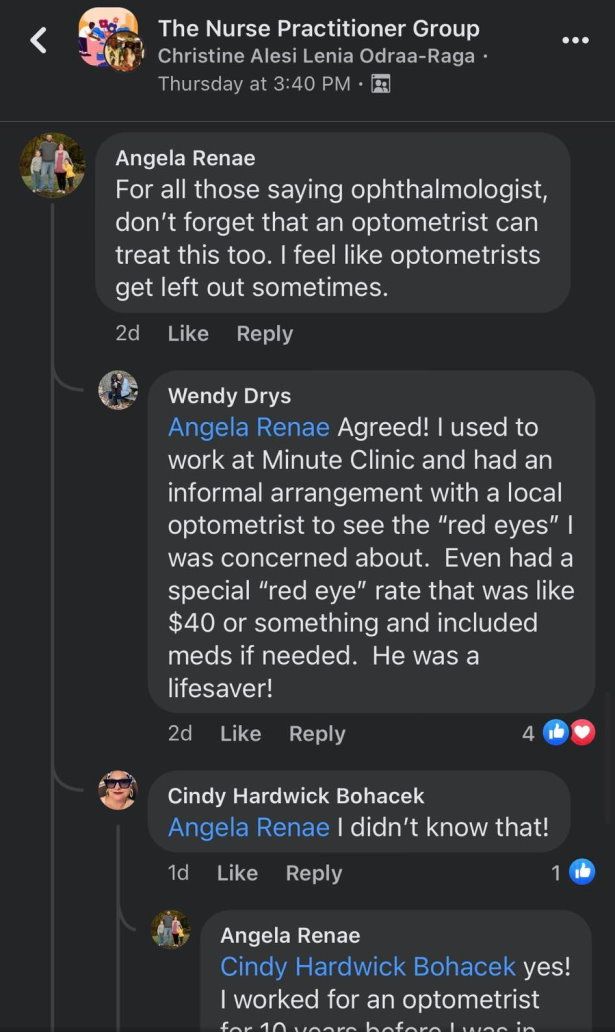
Last but not least, we have NP Angela Renae Tippitt reminding us (very wrongly) "that an optometrist can treat this too." God forbid we forget the optometrists, because "they get left out sometimes"! First of all, what the fuck is "this"? We haven't even established a definitive diagnosis yet! Referral to an optometrist, whose training is in no way comparable to that of an ophthalmologist who has gone through medical school and an ophthalmology residency, would be completely clinically inappropriate for an acute or emergent eye condition requiring medical or surgical management. And in any case, we certainly don't want to be caught anywhere near an incompetent midlevel trying to decide (incorrectly) whether a patient should be sent to an optometrist or an ophthalmologist. Who knows...maybe they do things differently over at the midlevel-infested US Department of Veterans Affairs, where NP Angela apparently works?
The real midlevel WTF, though, lies in NP Wendy Drys' revelation that when she used to work at a CVS MinuteClinic (presumably the one located in Leonardtown, Maryland, based on her NPPES record), she had "an informal arrangement with a local optometrist to see the 'red eyes' [she] was concerned about", an "informal arrangement" that apparently included a special "red eye" rate of $40. What in the actual fuck? We would certainly love to know more about what exactly this "informal arrangement" entailed. Was it mutually beneficial? For her sake, we certainly hope not. One has to wonder if Graceland University's 600-hour online FNP program teaches its students anything about state and federal anti-kickback statutes and the Stark law...